

Type: General Instruments
Hartmann Alligator Ear Forceps
Regular price
Rs. 919
Sale price
Rs. 919
Regular price
Rs. 1,380


Type: Instruments
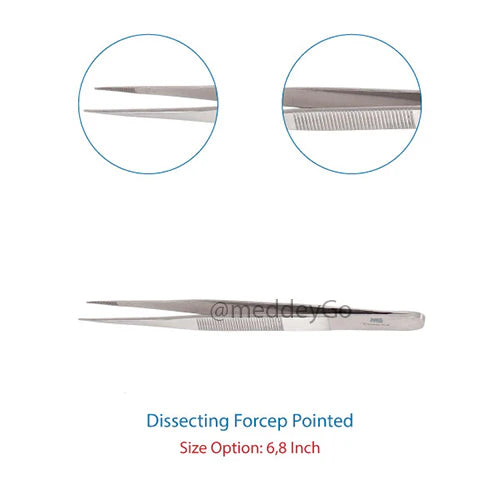
Dissecting Tissue Forceps Toothed
Regular price
From Rs. 247
Sale price
From Rs. 247
Regular price
Rs. 460


Type: Instruments
Artery Forceps Curved SS Delux Quality
Regular price
From Rs. 579
Sale price
From Rs. 579
Regular price
Rs. 828

Type: Instruments
Dissecting Tissue Forceps Plain
Regular price
From Rs. 247
Sale price
From Rs. 247
Regular price
Rs. 368


Type: General Instruments
Magill Forceps Stainless Steel Surgical Instrument
Regular price
From Rs. 689
Sale price
From Rs. 689
Regular price
Rs. 828

Type: General Instruments
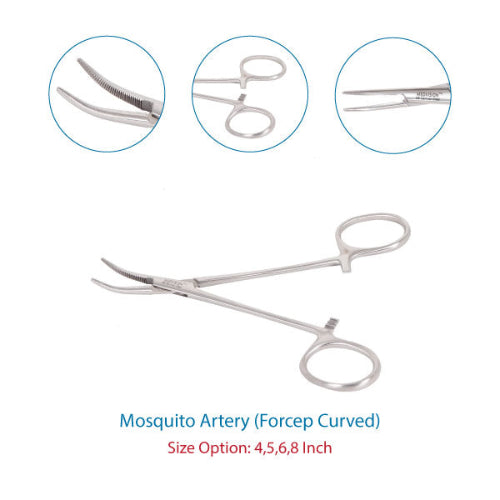
Mosquito Artery Forceps Curved 8 inch
Regular price
Rs. 380
Sale price
Rs. 380
Regular price
Rs. 506


Type: Instruments
Kochers Forceps Curved
Regular price
From Rs. 598
Sale price
From Rs. 598
Regular price
Rs. 920


Type: Instruments
Cervical Punch Biopsy Forceps
Regular price
Rs. 1,287
Sale price
Rs. 1,287
Regular price
Rs. 1,840

Type: General Instruments
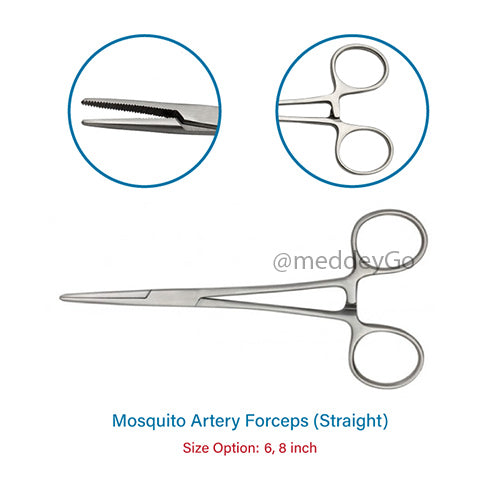
Mosquito Artery Forceps Straight
Regular price
From Rs. 395
Sale price
From Rs. 395
Regular price
Rs. 552


Type: Instruments
Crile Artery Forceps (Curved)
Regular price
From Rs. 597
Sale price
From Rs. 597
Regular price
Rs. 690

Type: Instruments
Allis Tissue Forceps Straight SS Delux Quality
Regular price
From Rs. 579
Sale price
From Rs. 579
Regular price
Rs. 736


Type: Instruments
Foerster Sponge Holding Forceps (Straight)
Regular price
From Rs. 706
Sale price
From Rs. 706
Regular price
Rs. 1,086

Type: Instruments
Allis Tissue Forceps Surgical Instrument
Regular price
From Rs. 413
Sale price
From Rs. 413
Regular price
Rs. 552


Type: Instruments
Kochers Forceps Straight
Regular price
From Rs. 598
Sale price
From Rs. 598
Regular price
Rs. 920

Type: Instruments
Bishop-Harmon Tissue Forceps SS
Regular price
Rs. 715
Sale price
Rs. 715
Regular price
Rs. 920